We apologise but unfortunately, we are no longer able to supply batteries from Milnrow Health Centre. You can contact us by phone or email (preferred) to request batteries or use the click and post service. For alternative places to collect batteries in person please see our Adult Hearing Aid Service Guide in the patient information leaflets section.
The Audiology Service offers hearing and aural therapy care for children and adults. Clinics are held in Rochdale, Middleton, and Heywood.
We assess and diagnose hearing loss and provide hearing aids for patients of all ages.
Diagnostic and rehabilitation sessions are provided for adults with tinnitus, balance and other more complex hearing related issues. Suction clearance of earwax is available for adults who cannot undertake routine ear syringing.
- We offer a Click and Post service – your hearing aid accessories (such as batteries and tubing) can be sent straight to your home. Click here to order. You can email us to request a telephone repair appointment – to save waiting on a busy phone line, email us your name, address, date of birth, the area you were issued your hearing aids (Oldham, Bury or Heywood, Middleton and Rochdale-HMR) along with a brief description of the problem and an audiologist will call you as soon as possible but always within 2 working days. Click here to email a telephone repair request.
- We are nationally accredited – our audiology services have received a national seal of approval from the prestigious United Kingdom Accreditation Service (UKAS). In accordance with UKAS schedule of accreditation.
- We are a dementia friendly service – our staff have received expert training to provide the very best care for people with dementia.
- We use top quality, modern and attractive digital hearing aids for adults and children – comparable to those offered by many private hearing care providers. The hearing aids are verified and using current best practice methods.
- We offer domically visits, for hearing aid patients that are housebound.
A day in the life of an audiology admin team member

What causes balance problems?
There are nerves running from the balance organ in the inner ear to the balance control centre in the brain along with various other inputs from the body. When all these inputs co-ordinate, balance is maintained. If there is a difference in these inputs, it is possible to experience a sensation of unsteadiness, dizziness or vertigo.
What can be done to help?
In the vast majority of cases, the symptoms do improve with time as the brain learns to cope with the changes that have taken place. However, depending on your symptoms, you may benefit from rehabilitation exercises or the Epley manoeuvre.
Bury and Heywood, Middleton and Rochdale Audiology have an Adult Balance service. A GP referral is required to access this service.
What can I expect to happen at the appointment?
Your appointment will last about one hour. You will usually be asked to complete a questionnaire prior to your arrival, which you will need to bring to your first appointment. During your appointment we will ask you about your dizziness and other relevant medical history. We may also assess your hearing and/or balance ability and you will have an opportunity to ask any questions throughout the consultation. You may bring one other person to the appointment with you and it is advisable not to drive immediately after the tests as you may feel a little unsteady.
What tests will be done?
If you have not been assessed previously, you will have a range of tests which the practitioner will explain to you. This may include tests of hearing, eye movements, balance assessment and tests for dizziness in certain positions. All these tests will help the practitioner identify any ear related causes for your dizziness.
Treatment
Rehabilitation exercises
If the brain fails to naturally recover from an episode of dizziness, simple exercises can be given which aim to improve your symptoms. These exercises may initially make your dizziness seem slightly worse, but if you continue with them your dizziness symptoms may gradually improve. If exercises are appropriate the practitioner will arrange a programme that is tailored to your particular problem.
The Epley manoeuvre
Sometimes dizziness can be experienced when moving in certain positions, such as when looking up or down, lying down or rolling over in bed. This is benign paroxysmal positional vertigo (BPPV) This is caused by loose particles triggering the sense organ in the inner part of the ear. If this is the cause of your dizziness, a simple but effective manoeuvre of the head undertaken by the practitioner can correct the problem.
What happens next?
The practitioner will discuss any test results with you and the options you have. Depending on your results we may recommend further investigations. We do not undertake any treatment or arrange ongoing management without your informed consent.
The practitioner who referred you to the service will be informed of the outcome of your appointment.
Exercises for Dizziness
The following exercises can help you to improve your balance and reduce symptoms of dizziness associated with movement. The exercises may initially make your symptoms seem slightly worse, but if you continue with the exercises your dizziness can gradually improve over time.
Benefit is usually achieved over a period of one to three months, providing the exercises are done correctly.
It is essential that you ensure the environment you are exercising in is safe. Make sure the area is clear and that there are no sharp edges or objects which could cause harm. For standing exercise’s, stand in a corner of the room and if you feel safer ask someone to stand in front of you or place a high back chair in front of you.
The exercises that the Audiologist recommends for you are listed in the booklet they have given you. Videos of these exercises are also available below. Repeat each exercise 3-4 times a day for up to 1 minute each. It is important you practice them every day. Gradually increase the speed and time you do each exercise to improve.
Exercise 1 Eye movement - Left and Right

Exercise 1 Eye movement - Up and Down

Exercise 2 Eye movement - Left and Right

Exercise 2 Eye movement - Up and Down

Exercise 3 Eye movement - Left and Right
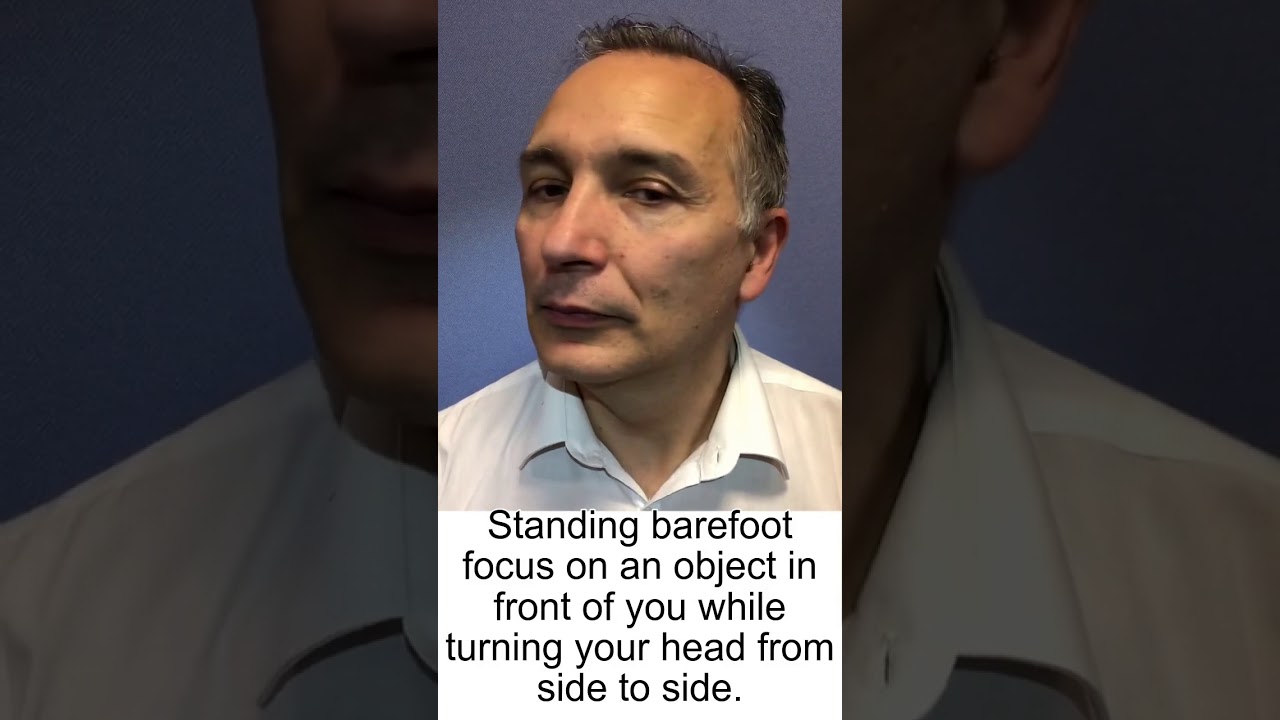
Exercise 3 Eye movement - Up and Down

Exercise 4 Eye movement - Left and Right

Exercise 4 Eye movement - Up and Down

Exercise 5 Eye movement - Left and Right

Exercise 5 Eye movement - Up and Down

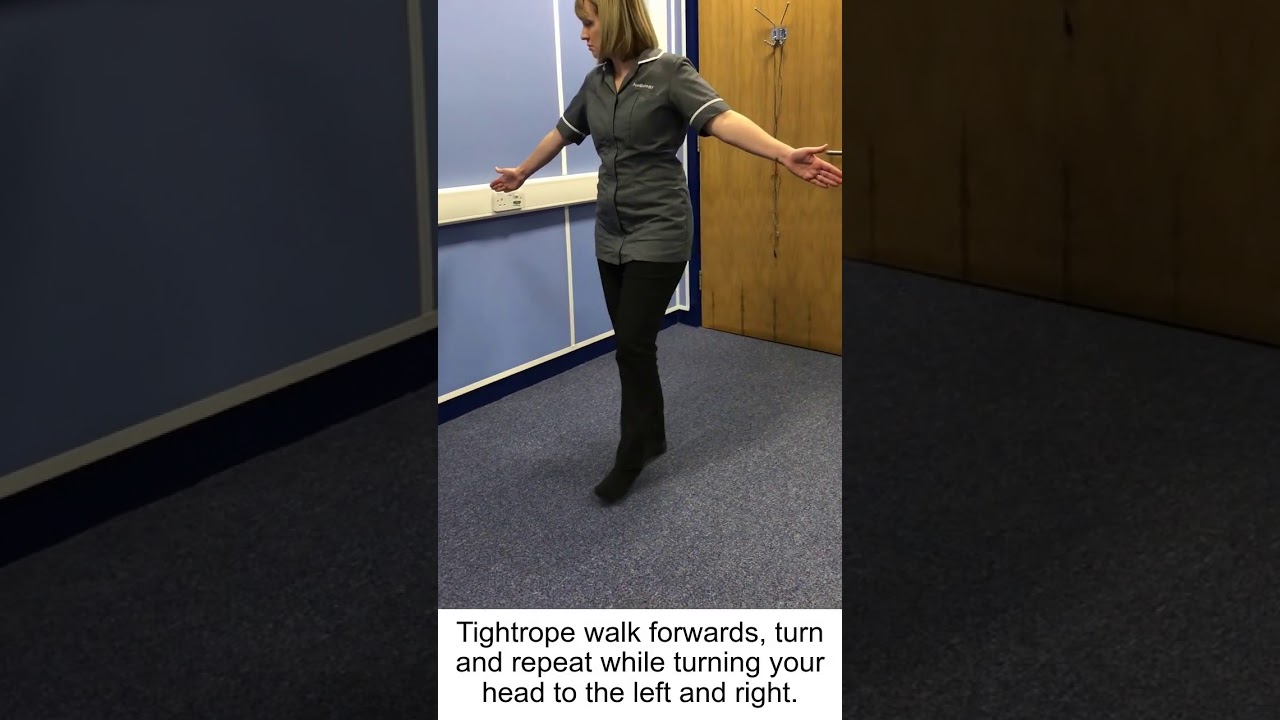
Exercise 6 Tightrope

Exercise 7 Tightrope 2
Exercise 8 Standing on one leg

Exercise 9 Tracing the alphabet

Exercise 11 Sitting down exercise

Exercise 12 Ball exercise

Exercise 13 Turning exercise

Exercise 14 Thai Chi Exercise

Exercise 15 Brandt Daroff

Exercise 16 - Epley right

Exercise 16 - Epley left

Exercise 17 - BBQ roll right

Exercise 17 - BBQ roll left

Olive Oil Use

The videos below provide practical demonstrations of the basics of hearing aid maintenance.
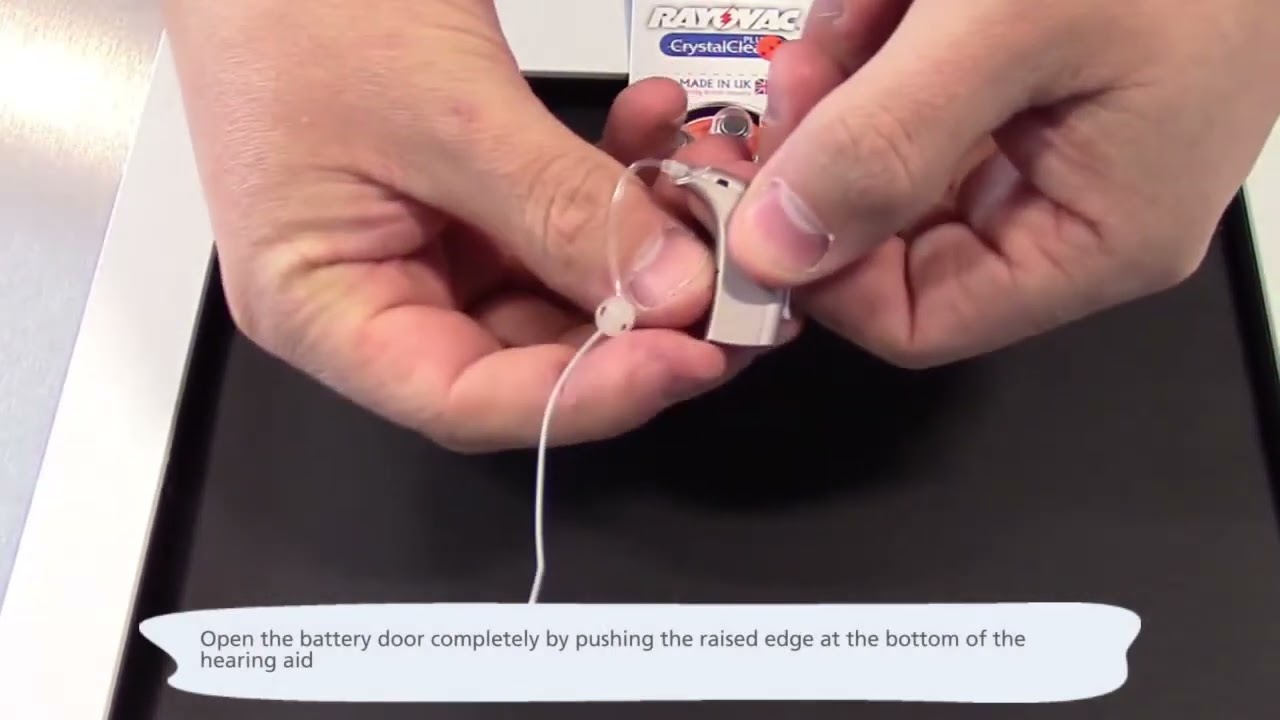
Changing the battery
Tube change - open fit
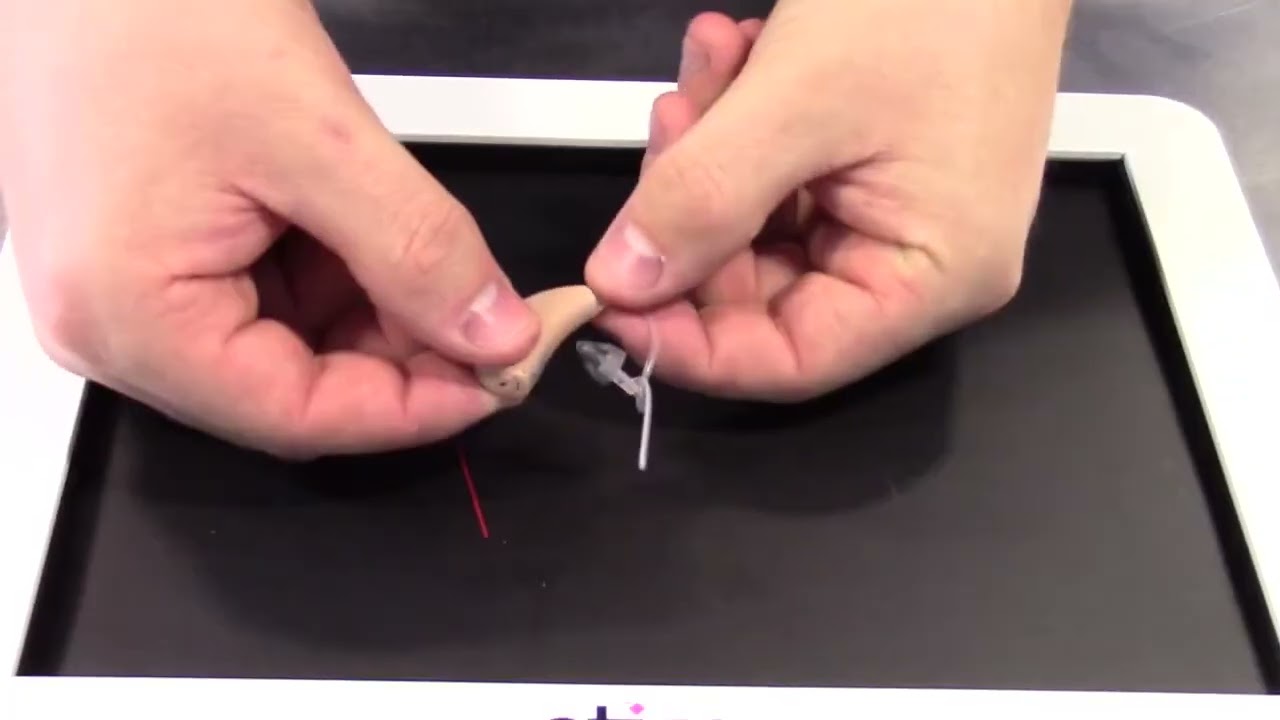
Tube change - ear mould
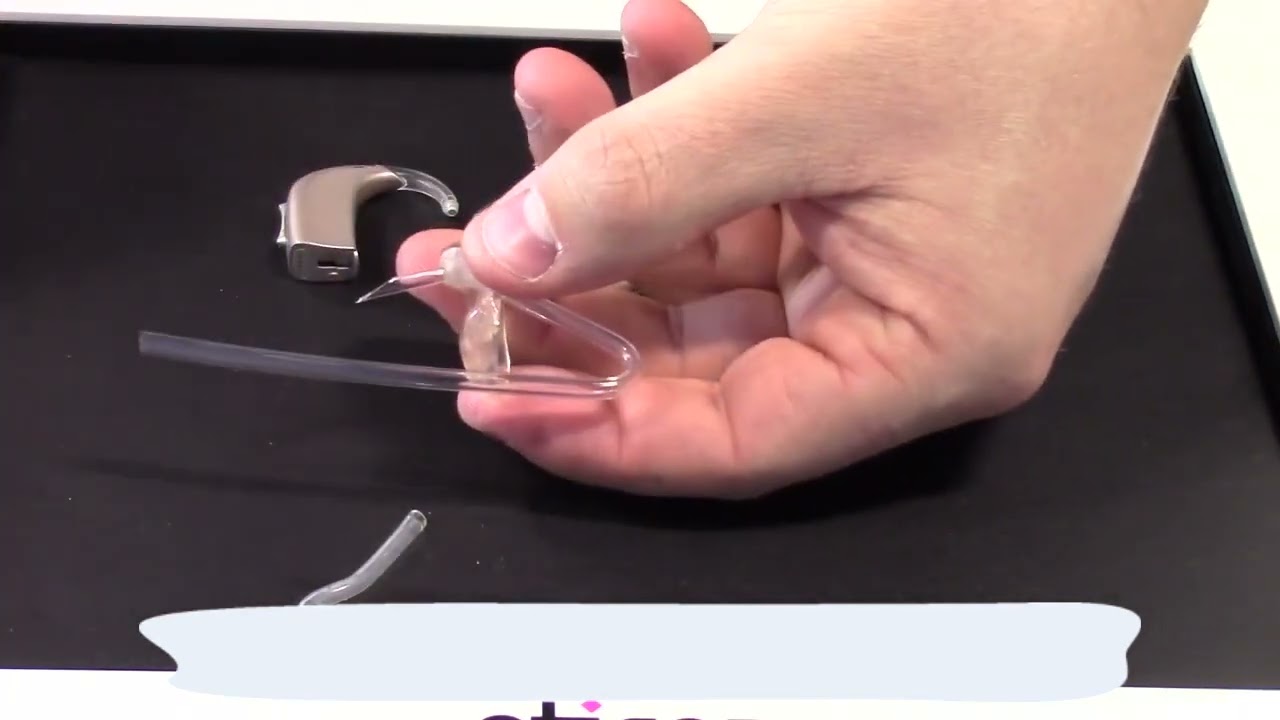
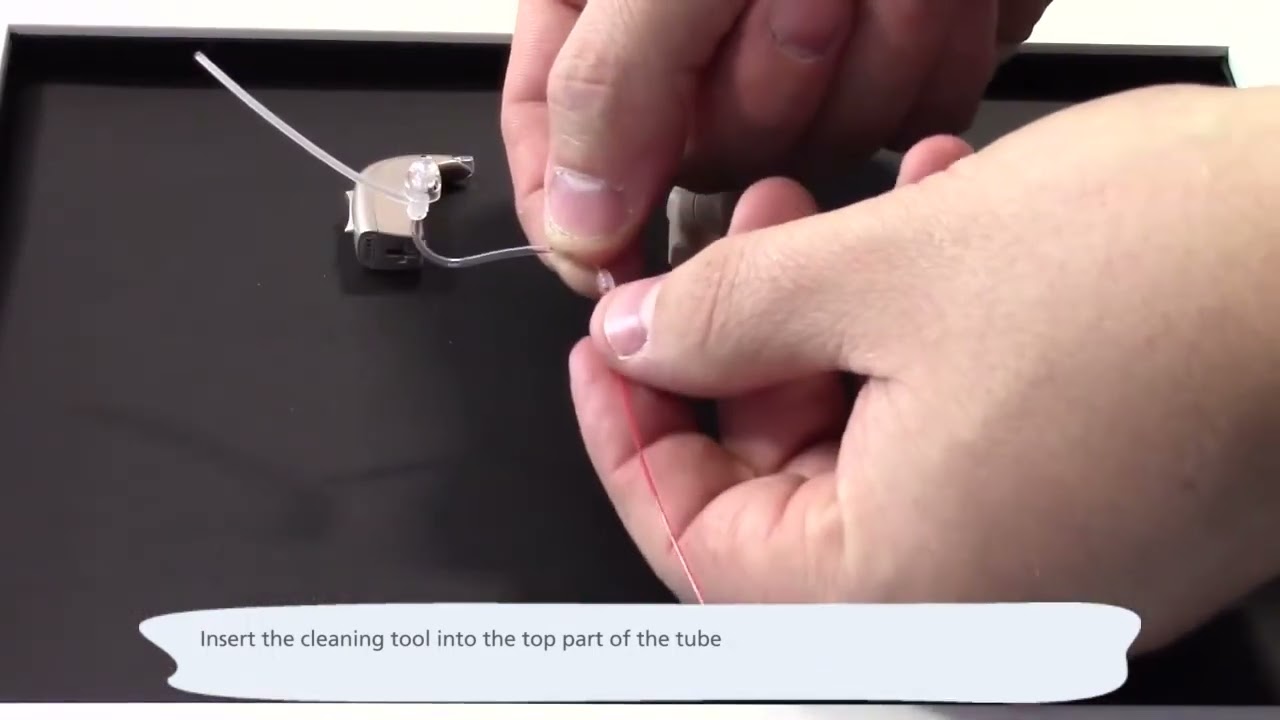
Tube cleaning - open fit
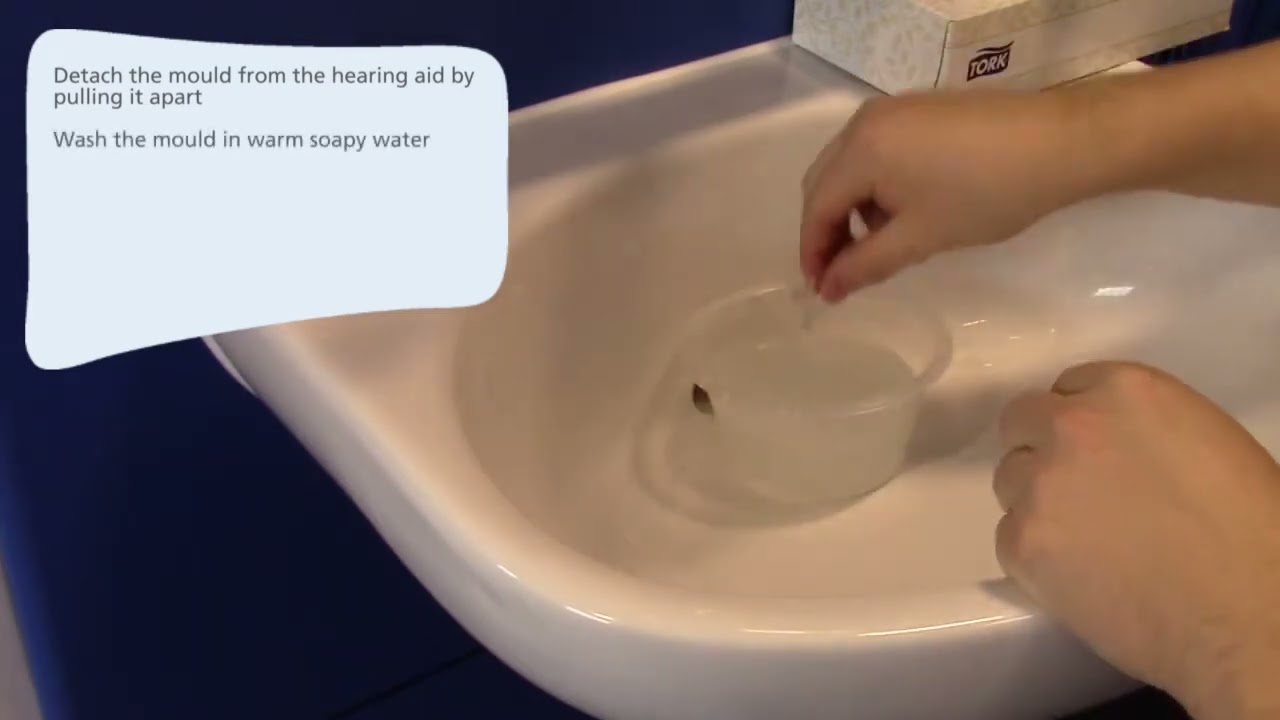
Cleaning the ear mould
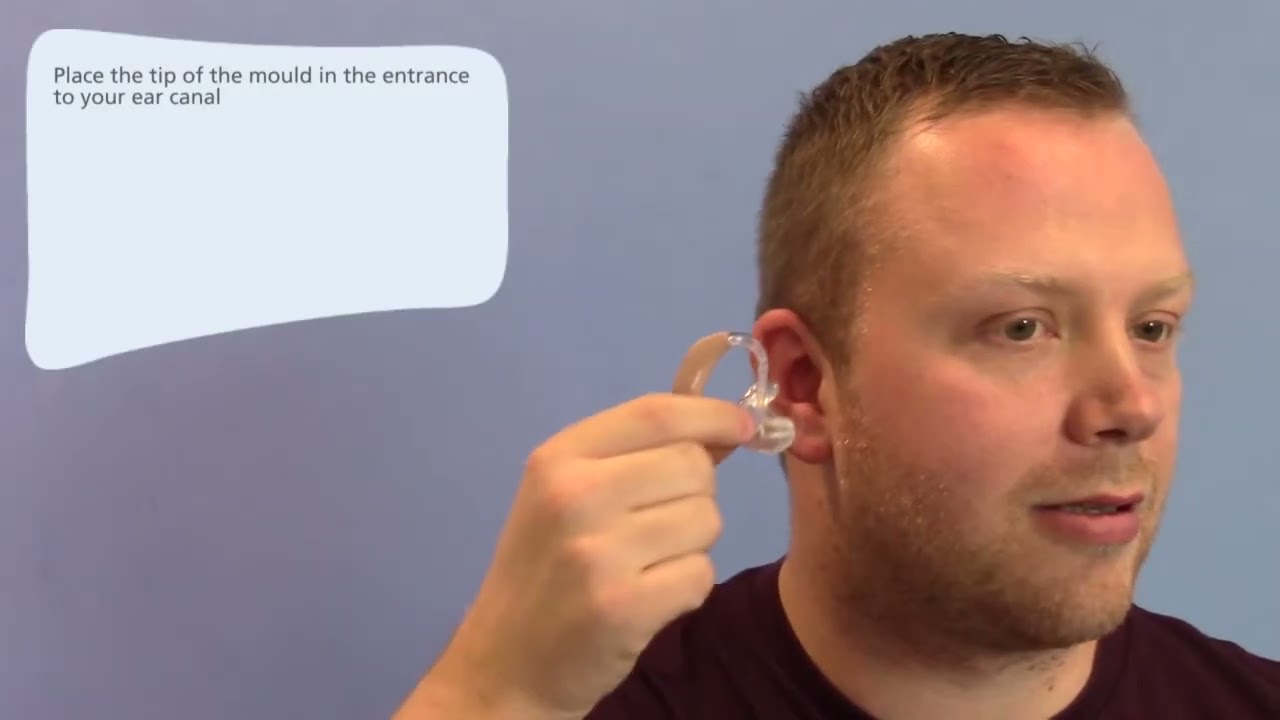
Putting the aid on - open fit
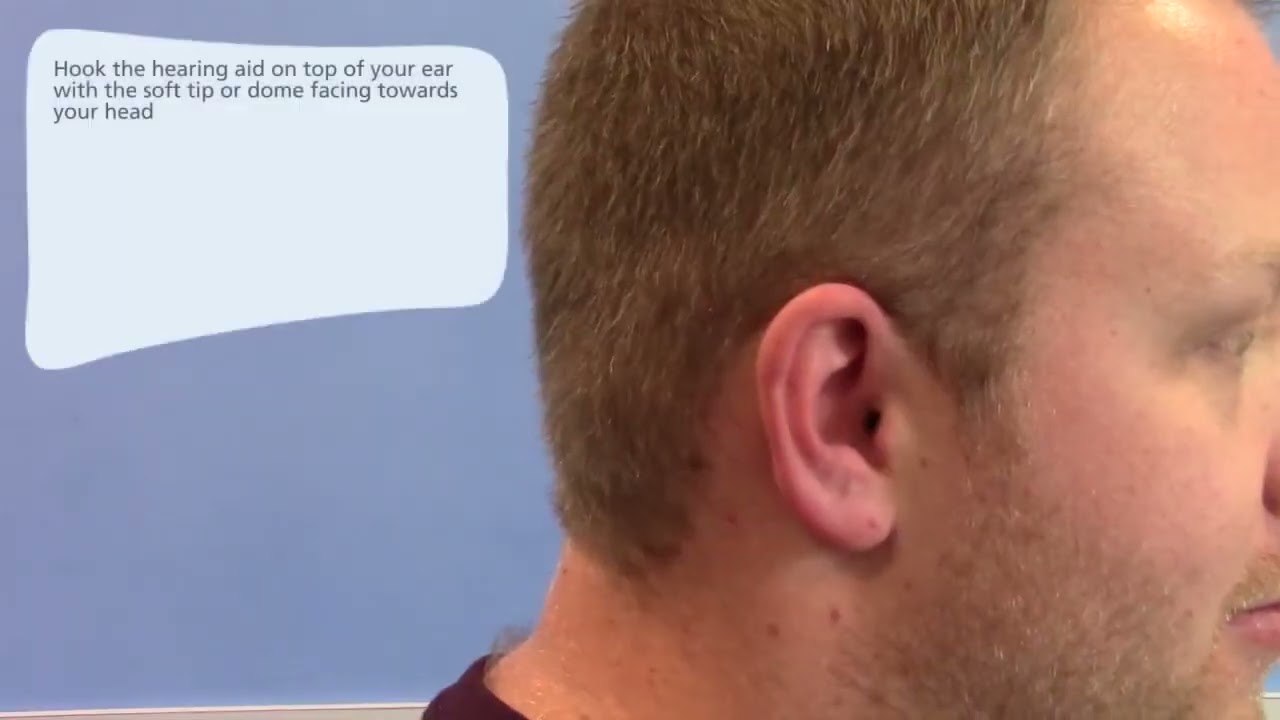
Putting the aid on - ear mould
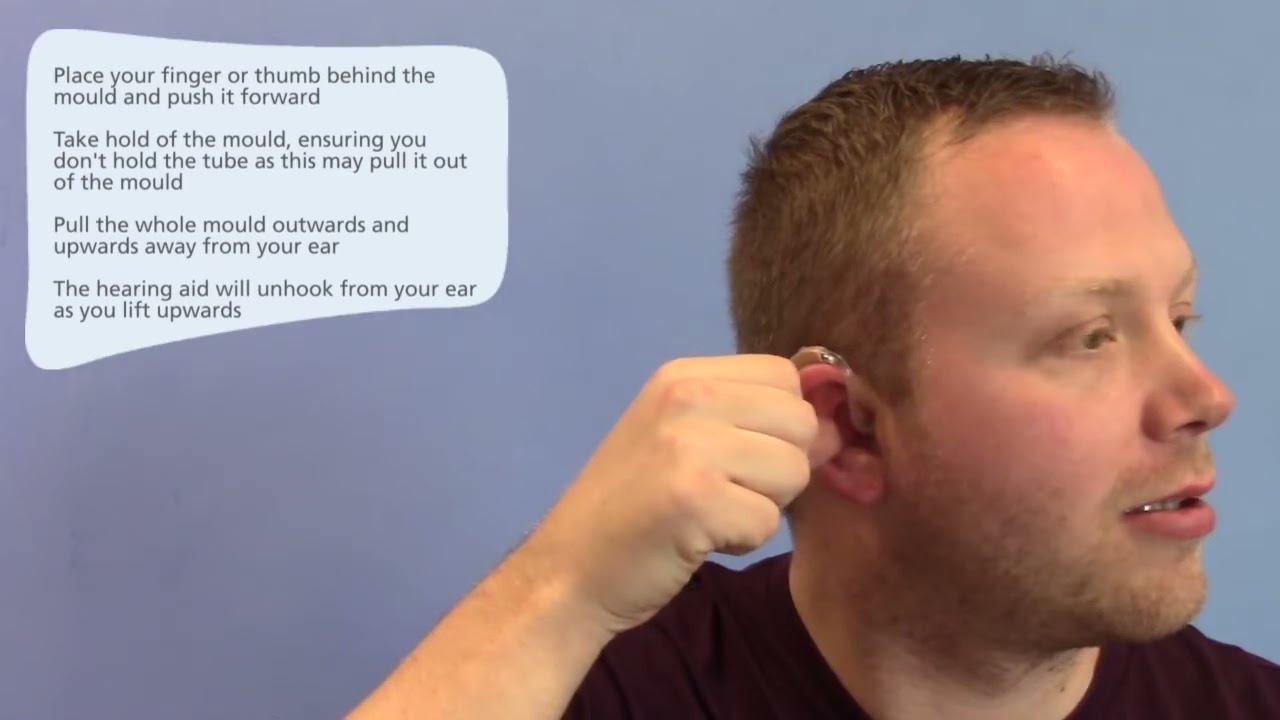
Removing your hearing aid
Virtual fitting packs
11 million people in the UK are living with a degree of hearing loss. It is estimated that this figure is going to rise over the next 20 years. There are many causes of hearing loss but the good news is that there is help and options available to you.
How do I know if I have a hearing loss?
Do you want the TV turned louder than other people? Are you missing parts of speech when out socialising or where there is a lot of background noise? Do you struggle to hear the teacher in the classroom? Do you often have to ask people to repeat themselves or completely get the wrong message? Is it hard for you to tell what the words are in the song or even cannot understand what they are saying when you turn the volume up on the radio or TV? Do you find that you are withdrawing from parties, stopped going out for a meal or to the cinema? If you have answered yes to any of these things then it is possible that you have some degree of hearing loss.
Getting help if you have a hearing loss
It is important to get your ears tested so you can find out if you have a hearing loss and what your options are to manage it.
Speak to your doctor and tell them your concerns. Your doctor will check your ears first and then make a referral to the Audiology department for tests to be performed. You should be able to get an appointment within 2 weeks at the Audiology department. You may be given a choice of where you want to have your Audiology Assessment. You can discuss these options with your GP.
If you are under 16 years old you do not need to speak to your doctor first. Your parent or your carer can contact your local Audiology department and make an appointment for some tests to be carried out.
What will happen at my hearing test?
You will be asked some questions by the Audiologist (the person who will be testing your ears). Some questions will be sent to you on a form that comes with you appointment letter. Please take time to answer any questions before your appointment and also write down questions that you would like to ask your audiologist.
First, the Audiologist will look into your ears. Next the Audiologist will instruct you on how to do a hearing test. You have to listen very carefully for the sounds, which will be played through some headphones that you will be wearing. The Audiologist will record your results on a chart known as an Audiogram.
After the test has been completed the Audiologist will discuss the results with you. They will also discuss treatment options and onward referrals if necessary. Onward referrals may include being referred for a scan or to see an ENT consultant. If you have chosen hearing aids as part of your treatment plan, the Audiologist will arrange for the aids to be fitted. Usually the hearing aids will be fitted within 2-3 weeks.
The following videos present some personal views from patients on their experience with the Audiology service and the benefits that being fitted with a hearing aid has brought them.






The NHS newborn hearing screening programme (NHSP) aims to identify moderate, severe and profound deafness and hearing impairment in newborn babies. Early identification of hearing impairment gives children a better chance of developing speech and language skills, and of making the most of social and emotional interaction from an early age.

The programme offers all parents in England the opportunity to have their baby’s hearing tested shortly after birth.
The incidence of significant permanent congenital hearing impairment (PCHI) is about 1 in 1,000 live births in most developed countries although this may be 3-4 times higher in certain communities or parts of the UK.
The most common reason for PCHI is loss of hair cells in the inner ear but it is sometimes due to malformation of the middle ear ossicles (small bones that transmit vibrations of the ear drum) or the ear canal (tube from the outer to the inner ear). If the hearing loss is due to a problem within the inner ear (sensory), or occasionally due to abnormalities in the hearing nerve (neural), the term sensorineural hearing loss is used. Hearing loss due to a problem within the middle ear or the outer ear is called a conductive hearing loss while a combination of sensorineural and conductive hearing loss is called a mixed loss.
In the event that your baby is referred to Audiology following a referral from the new-born hearing screening programme please use the link below offering advice and information regarding your visit to the Audiology department.
Your baby’s visit to the audiology clinic: information for parents click here.
Leaflet is available in other languages:
The HMR paediatric team provides a hearing aid service for children from new born until they transition to the Adult service.
Types of hearing loss
Permanent hearing loss
Hearing aids can be required from birth if a child is born with a permanent hearing loss, or they can acquire a permeant hearing loss after birth due to a number of reasons. We may offer further tests to see if we can find a cause for your child’s hearing loss.
Even a mild hearing loss can have an impact on a child’s speech, language and overall development. Establishing good hearing aid use as soon as possible from identification of a permanent hearing loss can significantly improve the outcomes for the child, including speech, language and overall development. The New born hearing aid screening program means we can identify a hearing loss within days of birth, so hearing aids can be fitted from as early as 4 weeks old.
https://www.ndcs.org.uk/information-and-support/first-diagnosis/
Hearing loss associated with middle ear fluid ( middle ear effusion)
Some children get temporary middle ear fluid that if causing significant problems with their hearing can impact on their speech, language and overall development. These children benefit from wearing hearing aids on a temporary basis to help overcome the hearing loss caused by the fluid. The hearing of the child is monitored and the aids can be adjusted to account for any fluctuations in hearing. When the hearing improves the hearing aids can be removed.
Your child may also be offered investigations into the cause of the hearing loss Deafness causes before birth | Deafness in childhood (ndcs.org.uk)
Understanding your child's hearing tests
Getting hearing aids
Hearing loss in children can range from mild to severe/profound but all can gain benefit from wearing hearing aids. The hearing aids come in a variety of colours and if the child is able we like them to choose the colour. We also offer ear moulds in a variety of colours or they can choose a picture from the brochure to go in the mould. Allowing the child to personalise their aid encourages them to want to wear them and be proud of the aids.
The hearing aid is programmed according to the child’s individual hearing loss, to help them hear every day sounds at a comfortable level and so they can hear speech as clearly as possible.
Sometimes the extent of a child’s hearing loss means they may benefit from cochlear implants and we can refer them on to the cochlear Implant Team for an assessment.
More information on hearing aids for children can be found in the NDCS booklet Hearing aids information for families:
Hearing aids information for families
Batteries and consumables can be requested through our click and post service. Click and Post Service (northerncarealliance.nhs.uk)
For hearing aid repairs an appointment can be made by contacting us on 01706 674 913 or NESaudiology@nca.nhs.uk
Hearing aids repairs can be by appointment or we offer a drop off and collect service.
Children will transition to the adult service aged 16. qs_transition_from_paediatric_to_adult_audiology_2011.pdf (ndcs.org.uk)
Teachers of the Deaf
The Paediatric Hearing Aid Team work closely with the Teachers of the Deaf from Local Educational Support Services for Hearing Impaired Children. Often a teacher from the Hearing Impaired Unit will attend the child’s initial hearing aid fitting and subsequent appointments. They can also support the child at home or in their educational setting.
Rochdale Additional Needs Service - Team for Children with a Hearing Impairment
Children’s Hearing Impaired Services Working Group (CHSWG) for Rochdale and Oldham.
We have a working group (CHSWG) for Rochdale and Oldham with the aim of ensuring the successful delivery of services for hearing impaired children and their families. Please see the leaflet in the link below for more information and how to get involved.
CHSWG Newsletter January 2021 - click here
Technology and hearing aids
Children can benefit from radio aids, especially in the school environment. They transmit the teachers voice directly to the hearing aid, this helps overcome background noise and poor classroom acoustics. They can also be useful in other situations such out-of-school activities. It can also be connected to other devices such as a smartphone or tablet. If suitable the radio aid will be provided by the teachers of the deaf.
Other devices can also be purchased such as streaming devices that link the hearing aids to smartphones, tablets etc. Loud or vibrating alarm clocks can help promote an older child’s independence.
Further information on all aspects of childhood deafness, hearing aids and technology can be found at The National Deaf Children’s Society (NDCS) website: https://www.ndcs.org.uk/
Useful links
National Deaf Children's Society | supporting deaf children (ndcs.org.uk)
How to use Oticon ON app | Bluetooth® hearing aids | Oticon
How to pair your hearing aid with a mobile phone (oticon.co.uk)
How to use an FM system in a classroom (oticon.co.uk)
How to use computer and tablet with your hearing aids (oticon.co.uk)
How to listen to music and audio with your hearing aids (oticon.co.uk)
Team for Children with a Hearing Impairment (Rochdale Additional Needs Service) | Our Rochdale
What is tinnitus?
Tinnitus is the term for the sensation of hearing a sound in the absence of any external sound. Symptoms of tinnitus are you may hear different types of sound, for example, ringing, whooshing or humming or buzzing in the ear. These can be continuous or they can come and go. The tinnitus might seem like it’s in one ear or both, in the middle of the head or even be difficult to pinpoint. Some people may think the noise is coming from outside and hunt for it until they discover it’s actually inside them!
Occasionally people have tinnitus that has a musical quality and can seem like a familiar tune or song. This generally occurs in older people who have a hearing loss and a strong musical interest. This type of tinnitus is known as musical tinnitus or musical hallucination.
Who gets tinnitus?
Tinnitus is very common and is reported in all age groups, even young children. About 30% of people will experience tinnitus at some point in their lives but the number of people who live with persistent tinnitus is approximately 13% (over 1 in 8). Tinnitus is more common in people who have hearing loss or other ear problems, but it can also be found in people with normal hearing.
The experience of tinnitus is different for different people. Most people find that they are able to continue their normal day-to-day activities. However, a small percentage of people with tinnitus report it as severely affecting them.
What causes tinnitus?
Whilst we do not know the exact answer to what causes tinnitus, we know that it is not a disease or an illness. It is generally agreed that tinnitus results from some type of change, either mental or physical, not necessarily related to hearing.
When we hear, sound travels into the ear and then the hearing nerves take the signals to the brain. The brain is then responsible for putting it all together and making sense of the sound. Because the ears don’t know what’s important and what’s not, they send a lot of information to the brain. This is too much information for us to process, so the brain filters out a lot of unnecessary ‘activity’ and background sound, such as clocks ticking or traffic noise.
If there is a change in the system, for example, a hearing loss or ear infection, the amount of information being sent to the brain changes. The brain then responds to this change in levels by trying to get more information from the ear, and the extra information you may get is the sound we call tinnitus. The tinnitus is therefore actually brain activity and not the ear itself! It is generally accepted that it isn’t only a change in the ear that can result in tinnitus, but it could be due to a change in our stress levels, for example, with tinnitus being noticed after periods of significant stress, a change in life circumstances or general wellbeing.
People often say that they are aware of noises in the ears when they have a cold, an ear infection or wax blocking the ear. Sometimes people become aware of tinnitus following a really stressful event and once they’re aware of it, seem to notice it more and more, but this usually fades once these things have passed. However, some people continue to notice the tinnitus, for example after an infection has cleared up.
Fortunately, tinnitus is rarely an indication of a serious disorder and a doctor will be able to check this for you.
What should I do?
The first person to talk to is your GP. You may need to be referred to an Ear, Nose and Throat (ENT) Surgeon or an Audiovestibular Physician, who will rule out any medical factors, assess your hearing and probably give you some information about what tinnitus is and how best to manage it. Some hospitals have hearing therapists or specially trained audiologists who are available to offer more support if you need it.
The most important thing to do is to keep doing the things you enjoy. If you start living your life differently to accommodate the tinnitus, it’s just going to seem more of a problem. You may need to do things differently, for example reading with some background music on, but it’s important that you do them nonetheless.
It does improve
When you first experience tinnitus, you may naturally be worried and very aware of this new sound. We constantly monitor our bodies and if anything changes, we become aware of the changes. Hearing tinnitus for the first time can be quite frightening if you think it means that something is wrong with you, or that it might change your life. It’s a new sensation and you need to give yourself time to adapt.
Most people find that their tinnitus does seem to settle down after this initial period, even without doing anything in particular. You might hear this being referred to as habituation. It’s a bit like walking into a room with a noisy fan or air conditioner. Initially, it seems really loud and then after a while, you stop noticing it as much. Tinnitus can often be much the same – initially, it’s more noticeable but you gradually notice it less than you did. The first time you realise it’s in the background is a great moment – it confirms that there are times when it’s less noticeable, which means you should be able to keep doing the things that you enjoy doing.
Things that can help
Talking to someone
People around you may not understand what tinnitus is and how it might affect you, so might not be able to give you the type of support you need. It can be really helpful to talk to someone who has experience of tinnitus.
Meeting people who have been through the same things you are going through right now can be very helpful. There are Tinnitus Support Groups around the country. Not only can you pick up tips from others, but you can gain (and give) support simply by sharing your story with people who understand because they’ve been there themselves.
Tinnitus UK offers a confidential tinnitus helpline.You can call us for support, and we may also be able to point you in the right direction for local support groups.
Relaxation
It is quite common to feel anxious and afraid when you first experience tinnitus. By relaxing more, you may be able to feel less stressed and so notice your tinnitus less. Learning to relax is probably one of the most useful things you can do to help yourself.
A really easy way to relax is to find somewhere peaceful and just slow your breathing down (feel free to have some sound on in the background). You can take a few slow deep breaths and pay full attention to the feeling of the breath entering your body, filling your lungs and leaving your body. When we use deep breathing to relax, we feel calmer and more able to manage the tinnitus, and often don’t notice it as much!
Using a hearing aid
Loss of hearing is often an unnoticeable and gradual process, and many people are surprised when they are told that they have a hearing loss. If you have hearing loss, using hearing aids can be helpful for tinnitus because they are restoring what you can’t otherwise hear.
Using sound
Tinnitus is usually more noticeable in a quiet environment. It’s a bit like candles on a birthday cake – in the lights, the candles aren’t very bright but if you turn the lights off, the candles seem much brighter. With tinnitus, when there is other sound, it doesn’t seem that loud, but when you turn all the other sound off, the tinnitus seems much more noticeable.
A lot of people have found that using background sound helps them – this can be a radio, music, or using natural sounds. People are really good at figuring out ways of making things better for themselves and you might already be aware that you generally don’t notice the tinnitus as much when there is background noise. By using sound at other times, you’re just using other ways of doing what you already know to be helpful.
Addressing sleep problems
People who live with tinnitus might have difficulty falling asleep or staying asleep. In order to sleep well, our bodies and our minds need to be relaxed. Worrying about the tinnitus, or worrying about how much sleep you’re getting (or missing out on), is unhelpful and will only make it more difficult to sleep. Most people with tinnitus sleep well and their tinnitus is no different from those who do not sleep well. People who have tinnitus and sleep poorly tend to worry more at night than people with tinnitus who sleep well. Working through problems during waking hours is better than in the middle of the night when you have nothing else to occupy you.
It helps to make use of relaxation techniques to prepare the body for sleep. Once your body and mind are relaxed, sleep will come a bit easier.
Having some soft sound in the bedroom can help some people with tinnitus sleep better. The type of sound you use is up to you – as long as it is pleasant or neutral.
Professional support
If you are referred to a specialist tinnitus clinic, and your tinnitus is particularly troublesome, you will be introduced to more formal or structured ways of managing tinnitus. Most centres use a combination of approaches. You may come across some terms before, or hear them when you get there, and it helps to have some understanding of what these terms are.
Cognitive Behavioural Therapy (CBT)
This is one psychological approach that can be useful in managing tinnitus. The idea is that when you became aware of your tinnitus, you responded to it negatively. For example, you may have thought there was something seriously wrong with your hearing (a belief) and this led to you being anxious (an emotion), and you then tried to feel better, for example by avoiding silence (a behaviour). Some beliefs and behaviours are helpful and that’s great – keep doing them! But some beliefs and/or behaviours are unhelpful and CBT helps you to recognise them, and then you work together with the clinician (usually a psychologist, audiologist or hearing therapist) to find different ways of responding to the tinnitus so it becomes less bothersome.
Mindfulness
This is a meditation technique that is used frequently for pain management, and more recently for tinnitus. The idea is that we tend to resist unpleasant sensations (eg hearing tinnitus). If we stop resisting and allow the unpleasant sensation, this alters our awareness to include more sensations. We start to notice that sensations become less dominant once our attention moves away from them and focuses on a different part of the body. All of this can change in a moment, simply by changing our awareness. If we use mindfulness effectively, we can create some space from the tinnitus and in that space, we can decide how we’re going to respond to it. It’s a wonderful way of achieving ‘peace and quiet’.
Tinnitus Retraining Therapy (TRT)
This is a very structured approach to managing tinnitus. Basically, TRT assumes that the tinnitus has been prioritised as an important signal. TRT uses sounds at a particular level to try to reduce the priority of the tinnitus so that you no longer hear it. It is based on the idea that we can get used to sounds, e.g. the sound of the fridge or air conditioner, so we can also get used to this sound of tinnitus. The process of getting used to the tinnitus sound is called habituation. TRT uses sound generators and counselling to attempt to retrain how the brain processes sound so that you habituate to the tinnitus. Most people working in the tinnitus field will use elements of TRT but the strict method is not frequently used because there is limited evidence for its effectiveness.
Take care of your hearing
Frequent, prolonged exposure to loud noise increases the risk of getting tinnitus, or of making it worse, so take care to avoid very loud sounds, or protect your ears against them. Wear proper ear protectors (not cotton wool) when hammering metal, using power tools or when you are near any noisy motors. Ear protection is also important if you watch live music or play in a band or orchestra. Ear protection should not be used if ordinary, everyday sounds are uncomfortable (this may be hyperacusis or oversensitivity to sound). If earplugs are worn for blocking out such sounds, it can actually make hyperacusis worse.
Hyperacusis
Hyperacusis is an increased sensitivity to sound. If you find that everyday or ordinary sounds are uncomfortable, you may have hyperacusis. Whilst it might seem natural to want to block out as much sound as possible, avoiding sound can actually make hyperacusis worse. Talk to your GP about this and ask for a referral to either an ENT Surgeon or Audiovestibular Physician who will be able to suggest management options – often, using sound (in a very controlled way) can improve hyperacusis.
More information
Having information about tinnitus can be very helpful. A lot of people start off looking online and while there is some fantastic information available on the internet, there is also a lot of very unhelpful information. An easy way to ensure what you are reading is appropriately written and produced is to check that the Information Standard has been adhered to - all our information complies with the Information Standard.
(Tinnitus UK, https://www.tinnitus.org.uk/all-about-tinnitus)
Aetiology - The cause of a condition (e.g. cause of the hearing loss).
Aided soundfield testing - A hearing test performed to check how well a person hears sounds of different frequencies when wearing hearing aids.
Auditory Brainstem Response (ABR) - This hearing test measures whether sound is being sent from the cochlea through the auditory (hearing) nerve to the brain. Three small sensors and a set of headphones will be placed on the child's head. For an accurate result, the child must be very still and quiet throughout the test.
Conductive deafness - When sound cannot pass efficiently through the outer ear and middle ear to the cochlea and auditory nerve.
Decibel (dB) - The unit used to measure the intensity or loudness of sound. Frequency - Most sounds are made up of different frequencies. Frequency is often thought of as the pitch of the sound. For example, on a piano keyboard, the keys to the left play low frequency (or low pitch) notes, and the keys to the right play high frequency (or high pitch) notes.
Hearing aid - Hearing aids amplify sound. Modern hearing aids process sound using digital technology.
Inserts - A type of headphone that inserts into the ear to present sounds during a hearing test.
McCormick toy test - A hearing test used in which the child must discriminate between similar speech sounds in words.
Middle ear - The middle ear is made up of the ear drum which vibrates because of sound waves, and three tiny bones known as the ossicles which pass on these vibrations to the inner ear.
Otoacoustic emissions (OAE) - This hearing test is commonly used as part of the screening tests carried out on babies shortly after birth. It tests the cochlea response. A small earpiece is placed in the child's ear and a clicking sound is played. If the cochlea is working properly, the earpiece will pick up the response and it is recorded on a computer.
Phoenix - Automated version of the McCormick Toy Test.
Pure Tone Audiometry (PTA) - Behavioural test which actively involves children from the age of three years. Sounds are played through headphones or earphones placed inside the child's ear to test each ear separately. Younger children might be shown how to move a toy each time they hear a sound and older children might be asked to respond to sounds by saying "yes" or pressing a button.
Radio aid - A radio aid consists of a transmitter (used by the person who is talking) and a receiver (used by the deaf child/adult). A microphone picks up the speaker’s voice.The sounds are then transmitted by radio waves to the receiver.
Sensorineural deafness - This is a permanent hearing loss. The inner ear isn’t working properly, so the cochlea or hearing nerve don’t work as they should.
Soundfield Performance Test - Behavioural test where sounds are played through speakers to test the child’s overall hearing rather than each ear separately. Children are shown how to move a toy each time they hear a sound.
Tympanometry - Tympanometry is not a test of hearing; it is used to check how well the moving parts of the middle ear are working If the eardrum is not moving freely, there is likely to be some fluid or another problem with the middle ear.
Visual Response Audiometry (VRA) - This can test the full range of hearing but does not give specific information about each ear. An audiometer plays sounds of different frequencies and loudness through speakers. When the child hears the sound, they will turn their head when a visual "reward" is activated, such as a toy lighting up.
Glossary of hearing aid-related terms
Datalogging - A program on the hearing aid that monitors how much the hearing aid is being worn.
DSL version 5 - Prescription that the hearing aid is set to.
Earmould/mould - An earmould is the part of the hearing aid that fits into the ear.
Feedback - When sound leaks out from the ear mould and causes whistling.
Linear - Loud sounds are amplified the same as quiet sounds.
RECD - A measurement performed that takes into account that size and shape of your child’s ear when setting the hearing aid.
Soundrecover - A setting that helps make high frequency sounds more audible. Whistleblock technology - Hearing aid setting that reduces feedback.
Wide Dynamic Range Compression (WDRC) - Sounds are amplified by different amounts depending on how loud they are to start off with. Quiet sounds are amplified more while loud sounds are not amplified as much.
Clinic Details
All clinics are accessed by booked appointment only. Appointments can be made by telephone or email.
- Nye Bevan House, Maclure Road, Rochdale, OL11 1DN Free parking available. Short walk from tram stop and Rochdale train station.
- Durnford Street Clinic, 2 Durnford Street, Middleton, M24 5UD. Roadside parking available.
- Langley Clinic Borrowdale Rd, Langley, Middleton, M24 5QG. Roadside parking available.
- Phoenix Centre, Church Street, Heywood, OL10 1LR. Free car park and roadside parking available.
- Croft Shifa Health Centre Belfield Road, Rochdale, OL16 2UP. Free car park and roadside parking available.
The Traveline journey planner website can help you to plan your route using public transport.
Please click on the links below to find information on the AccessAble website about each of our clinics
Below are some videos showing you what your visit to the clinic will look like. This can be helpful if you are anxious about new experiences.
Adults can be referred by a GP or an ENT Consultant. Children can be referred by a range of health professionals and parental referral is also accepted.
- National Deaf Children's Society (NDCS) http://www.ndcs.org.uk
- British Tinnitus Association(BTA) http://www.tinnitus.org.uk
- Action on Hearing Loss http://www.actiononhearingloss.org.uk
- Hearing Link http://www.hearinglink.org